
02 Jan Spinal Cord Injury and Bowel Management.
Bowel Management is an important every day task for participants with Spinal Cord Injury. Main Changes to bowel function due to spinal cord injury occur in lower section of the digestive tract – the large intestine, rectum and anus. Changes to the nerve supplying the muscles of large intestine wall result in a decreased push effect in the bowels. Thus it now takes longer for the faeces to work its way around the bowel. As the poo (faeces) is now staying longer than needed in the large bowel. Large intestine has plenty of time to drain out more than usual fluid from the faeces making it harder which results in Constipation. Changes in moistness which is found to occur post spinal cord injury causes decrease in lubrication, and further slows down the transit of faeces around the bowel which is constipation.
Accidents – changes to the nerves supplying the muscles in the rectum and anus can result in an inability to predict or control bowel movements.
These changes which cause Constipation and accidents are referred to as Neurogenic bowel.
How to manage Neurogenic Bowel effectively?
To be able to manage these changes, it is important to observe and understand what type of bowel you have after injury. Mainly there can be two types of bowels noticed.
- Reflexive Bowel
- Flaccid Bowel
Management of these bowel types differs significantly. If you are unsure of which type of bowel, talk to your Integral Home Care Community Nurse.
Lower Motor Neuron (LMN) bowel – Flaccid bowel occur in people with spinal cord injuries at or below the T12/L1 level. The reflex action which contracts the muscles around the anus and rectum does not occur leading to
- Poor or no anal tone
- Loss of voluntary control
- Poor or no sensation of lower bowel
- Decreased peristalsis
Note: Impacted bowel or Constipation can cause Autonomic Dysreflexia in people with Spinal Cord Injury.
The Management:
Good Bowel Routine -> Effective and predictable Emptying -> Social Continence
Right Time:
The Bowel needs to be retrained to empty at a regular and consistent time each day. Choose a time which works for you :
- Before work
- Previous bowel habit prior to injury
- Availability of Care Support
Flaccid bowel can be managed once or twice a day with an average of 15-30 mins of time spent on the toilet.
Right Place:
You won’t get a result if the poo (stools) is sitting up in the large bowel. Thus it is important to use a bowel stimulant like Senna or Bisacodyl tablets. These medications work by stimulating movements (peristalsis). It takes 10-16 hours for these tablets to get the poo to rectum if no other issues involved. So, adjust the timing of taking these tablets to suit your routine.
For Example:
- If you wish to toilet at 8am, the Senna tablets should be given at approximately 8pm the night prior.
- If you are having accidents prior to getting over the toilet (8am), try taking the tablet a bit later.
- If you have to sit on the toilet 1 hr before a result, try taking the tablet earlier.
- If you are toileting twice a day, but only taking Senna once a day, you should expect a better result for the toileting episode10-16 hours after taking the Senna – Larger morning result, less in the evening.
Right Amount:
Daily Monitoring of the results of bowel routine provides a ‘checks and balances’ system to ensure that your bowels are on track, and early warning if things are starting to go wrong. Our body makes poo every day but the amount of poo is directly proportional to what we eat and how much we eat.
Fibre is a cellulose product found in plant foods that cannot be digested by our bodies – which is then eliminated in our poo/faeces.
Soluble Fibre – Soaks up the water and helps form the stool/poo. Soluble fibre passes in our gut much slower compared to Insoluble fibre, which in turn leads to constipation. Thus in Spinal Cord Injury participants, it is recommended to have 15g of soluble fibre instead of the 30g usual recommendation. Foods like bran, breads, and cereals possess soluble fibre.
Insoluble fibre – Insoluble fibre doesn’t soak up water thus passes through the gut more easily and also quickly. Its mostly found in fruits, nuts, and seeds but excess consumption can lead to diarrhoea. In addition its quick passage through the gut can influence the ‘The Right Place’ of bowel Management.
Right Consistency:
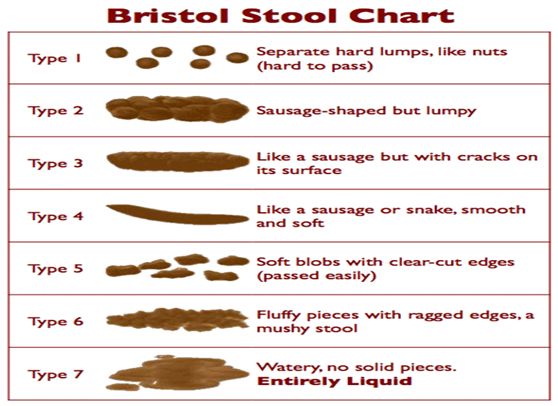
The consistency of the poo/stool is mainly dependent on how much water has been lost during the transit of poo in the bowel. Aim type 2 or type 3 on Bristol stool chart especially for the flaccid bowel type. Soft stools are harder to empty out of the rectum compared to firmer stools. Pooling of soft stools in the rectum can lead to accidents. Firmer type 2-3 stools/poo are easier to remove to ensure some peace of mind through the day.
Important Triggers:
Gastro-Colic Response: An increase in the contractile waves of the bowel are generated after filling the stomach with either food or a warm drink. Gastro-Colic reflux is usually strongest in the mornings.
Exercise: Exercise stimulates peristalsis, exercise can also help with controlling pain levels in the body which in-turn help with preventing constipation as it cuts down on usage of pain medication.
Things to remember- Bowel Management

Keep Active – Increases bowel movements and helps with pain management.

Try to have breakfast or a warm drink before getting on the toilet- Gastro-Colic reflux triggers bowel movements helping defaecation.

Everyone is different – Getting your timing right. Aperients might take 10-16 hours to get the poo to the rectum ready for emptying. Adjust timings depending on results in the following day.

- Drink at least 2 lit of water a day
- Know the difference between soluble fibre and Insoluble fibre
- Have a balanced diet – Food you eat does impact your bowel regimen
- Try to cut down on drinks (e.g. coffee) and foods that contribute to constipation.
- Keep a bowel diary, knowing your bowel needs a picture of a month and every day is not the same.
- Document type of stool formed – Bristol Stool chart for consistency.
- Type 2-3 is recommended in spinal-cord injury.
- Remember bowel management is an ongoing process, a trial and error process which needs continuous supervision in Spinal Cord injury participants.